One of the main causes of home air pollution, especially in developing nations, is the use of solid biomass fuels (wood, crop leftovers, animal dung, and coal) for cooking and heating. This has serious negative impacts on respiratory health. Chronic obstructive pulmonary disease (COPD), chronic bronchitis, asthma, and acute lower respiratory infections (ALRI) are all closely associated with long-term exposure to high amounts of particulate matter (PM2.5) and carbon monoxide (CO) from these fuels. The purpose of this study was to examine the Influence of biomass solid fuel usage on incidences of respiratory symptoms amongst women adopters of ICS in Nakuru town East suburbs. The study was informed by energy stacking and theory of subsidy. The study utilized mixed method research design. Data were collected from 315 female heads from of households that had adopted ICS, two FGD and key informant interviews. Sampling techniques utilized were multi-stage cluster sampling for the women heads of households while purposive sampling was used to select KIIs and participants in the FGDs. Quantitative data was analyzed using descriptive statistics and logistic regression. Qualitative data was content analyzed. Study findings revealed that 67.8% of households relied on charcoal, while 54.9% used firewood, often alongside ICS. Households that predominantly used firewood reported the highest incidence of respiratory symptoms, highlighting the persistent dangers of solid fuel combustion. Logistic regression analysis demonstrated that women in firewood-dependent households were 2.43 times more likely to experience respiratory related symptoms than those using charcoal.
| Published in | World Journal of Public Health (Volume 11, Issue 1) |
| DOI | 10.11648/j.wjph.20261101.20 |
| Page(s) | 78-91 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Biomass Solid Fuels, Women, Respiratory Related Symptoms, Improved Cooking Stoves, Kenya
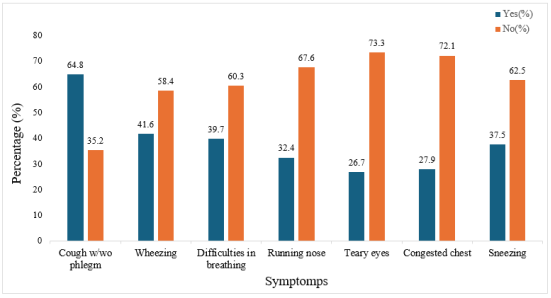
Reported incidence/Symptom | YES - F (%) | NO -F (%) |
|---|---|---|
Cough with/without phlegm | 204 (64.8%) | 111 (35.2%) |
Wheezing | 131 (41.6%) | 184 (58.4%) |
Difficulties in breathing | 125 (39.7%) | 190 (60.3%) |
Running nose | 102 (32.4%) | 213 (67.6%) |
Teary eyes | 84 (26.7%) | 231 (73.3%) |
Congested chest | 88 (27.9%) | 227 (72.1%) |
Sneezing | 118 (37.5%) | 197 (62.5%) |
Variable | Category | F (%) |
|---|---|---|
Uses firewood - ever uses firewood | Yes | 173 (54.9%) |
No | 142 (45.1%) | |
Mainly uses Charcoal | Yes | 272 (86.3%) |
No | 43 (13.7%) | |
Used charcoal for cooking today | Yes | 210 (66.7%) |
No | 105 (33.3%) | |
How easy to find a charcoal vendor | Not easy | 14 (4.4%) |
Somewhat easy | 61 (19.4%) | |
Very easy | 240 (76.2%) |
Coughing with/without phlegm | Wheezing | Difficulties in breathing | Runny nose | Teary eyes | Congested chest | Sneezing | ||
|---|---|---|---|---|---|---|---|---|
Explanatory variable | OR | OR | OR | OR | OR | OR | OR | |
Ever uses firewood | (No) | |||||||
Yes | 0.642 | 0.480** | 1.270 | 0.618** | 1.067 | 1.100 | 0.690 | |
Main type cooking fuel-Charcoal | (No) | |||||||
Yes | 0.988 | 0.696 | 0.965 | 1.029 | 0.496** | 1.330 | 0.571 | |
Used charcoal for cooking today | (No) | |||||||
Yes | 0.775 | 1.300 | 0.979 | 1.329 | 1.567 | 1.051 | 1.892** | |
How easy to find a charcoal vendor | (Not easy) | |||||||
somewhat easy | 1.170 | 2.688 | 0.519 | 1.413 | 1.651 | 0.732 | 0.502 | |
very easy | 1.584 | 2.707 | 0.516 | 1.128 | 1.264 | 0.590 | 0.452 | |
Access to charcoal is a challenge | (No) | |||||||
Yes | 2.599* | 0.859 | 0.654 | 1.005 | 1.032 | 1.942 | 0.653 | |
Note. Estimates represent the log odds of "Binary Indicator = No vs. Yes" Reference category in bracket *Significant at 0.1, ** significant at 0.05, *** significant at 0.01 | ||||||||
ALRI | Acute Lower Respiratory Infections |
COPD | Chronic Obstructive Pulmonary Disease |
COR | Crude Odds of Respiratory Illness |
CO2 | Carbon Dioxide |
HAP | Household Air Pollution |
FEV | Forced Expiratory Volume |
FGD | Focus Group Discussions |
FVC | Forced Vital Capacity |
LMICs | Low- And Middle-Income Countries |
IAP | Indoor Air Pollution |
ICS | Improved Cooking STOVE |
KII | Key Informants Interviews |
LPG | Liquefied Petroleum Gas |
OR | Odds Ratio |
PM2.5 | Particulate Matter |
SAA | Sub-Saharan Africa |
WHO | World Health Organization |
| [1] | Acharya Bikram, & Marhold Klaus (2018). Determinants of household energy use and fuel switching behavior in Nepal. Elsevier ltd, 169 (2019), 1132-1138. |
| [2] | Adane, M. M., Alene, G. D., Mereta, S. T., & Wanyonyi, K. (2020). Prevalence and Risk factors of Acute Lower Respiratory Infection Among Children Living in Biomass Fuel Using Households: A community-based cross-sectional study in Northwest Ethiopia. BMC Public Health, 20(363), 1-13. Energy Research & Social Science, 89, 102546. |
| [3] | Adewuyi, E., James, O., & Adebayo, B. (2024). Household energy use and women’s respiratory health in urban Nigeria: A cross-sectional analysis. Journal of Environmental and Public Health, 18(2), 113-128. |
| [4] | Ahmed, M. (2021). Gender and climate justice in clean cooking transitions. African Journal of Environmental Policy, 10(1), 33-44. |
| [5] | Alexander, D., Linnes, J. C., Bolton, S., & Larson, T. (2014). Ventilated cookstoves associated with improvements in respiratory health-related quality of life in rural Bolivia. Journal of Public Health, 36(3), 460-466. |
| [6] | Azanaw, J., & Endalew, M. (2025). Solid fuel use and household air pollution in Sub-Saharan Africa: Analysis of Demographic and Health Surveys. PLOS Global Public Health, 3(1), e0002145. |
| [7] | Baltramo, T., et al. (2019). Efficient fuel stoves, fuel use patterns and particulate matter in Uganda. Energy Economics, 84, 104518. |
| [8] | Begum, B. A. (2015). Particulate matter emissions from improved cookstoves and traditional cookstoves in Bangladesh. Journal of Health and Pollution, 5(9), 23-30. |
| [9] | Carrión, Seyram Kaali, Patrick L. Kinney, Seth Owusu-Agyei, Steven Chillrud, Abena K. Yawson, Ashlinn Quinn, Blair Wylie, Kenneth Ae-Ngibise, Alison G. Lee, Rafal Tokarz, Luisa Iddrisu, Darby W. Jack, Kwaku Poku Asante (2019). Examining the relationship between household air pollution and infant microbial nasal carriage in a Ghanaian cohort. Environment International, 133, |
| [10] | Clark ML, Peel JL, Balakrishnan K, Breysse PN, Chillrud SN, Naeher LP, Rodes CE, Vette AF, Balbus JM. (2013). Health and household air pollution from solid fuel use: the need for improved exposure assessment. Environ Health Perspect. 121(10), 1120-8. |
| [11] | Dida, G. (2022). Indoor air pollution, maternal health, and gender inequalities in Kenya. East African Medical Journal, 99(2), 33-44. |
| [12] | Foote, M. E., Gieraltowski, L., Ayers, T., Sadumab, I., Sitnal, H., Silk, J. A., Were, V., Hughes, J. M., & Quick, R. E. (2013). Impact of Locally-Produced, Ceramic Cookstoves on Respiratory Disease in Children in Rural Western Kenya. The American Society of Tropical Medicine and Hygiene, 88(1), 132-137. |
| [13] | Fullerton, D. G.; Suseno, A.; Semple, S.; Kalambo, F.; Malamba, R.; White, S.; Jack, S.; Calverley, P. M.; Gordon, S. B. Wood smoke exposure, poverty and impaired lung function in Malawian adults. Int. J. Tuberc. Lung Dis. 2011, 15, 391-398. |
| [14] | Gatari, M. J., & Kinney, P. L. (2023). Household air pollution in Kenya: Patterns, determinants, and respiratory impacts among women. Environmental Research, 222, 115-128. |
| [15] | GOK. (2021). National Strategic Plan for Prevention and Control of Non-Communicable Diseases 2021/22—2025/26. Department of non-communicable diseases. |
| [16] | Hasan, M., Tasfina, S., RaysulHaque, S. M., Saif-Ur-Rahman, K. M., Khalequzzaman, M., Bari, W., & Islam Sharifu, S. (2019). Association of biomass fuel smoke with respiratory symptoms among children under 5 years of age in urban areas: Results from Bangladesh Urban Health Survey, 2013. Environmental Health and Preventive Medicine, 24(65), 1-10. |
| [17] | Holden, K. A., Lee, A. R., Hawcutt, D. B., & Sinha, I. P. (2023). The impact of poor housing and indoor air quality on respiratory health in children. Breathe, 19(58), 1-11. |
| [18] | International Energy Agency. (2024). Africa Energy Outlook 2024: Clean Cooking and Energy Access Pathways. International Energy Agency. |
| [19] | International Energy Agency (IEA). (2022). Africa energy outlook 2022. Paris: International Energy Agency. |
| [20] | James, S. B., Shetty, R., Kamath, A., & Shetty, A. (2020). Household cooking fuel use and its health effects among rural women in southern India—A cross-sectional study. PLoS ONE, 15(4), 1-12. |
| [21] | Kimani, E., Mutheu, S., & Wanjiku, R. (2023). Indoor air pollution and adolescent respiratory health in Kenya: A cross-sectional multi-county study. African Journal of Respiratory Medicine, 15(2), 54-67. |
| [22] | KNBS and ICF. 2023. Kenya Demographic and Health Survey 2022: Volume 1. Nairobi, Kenya, and Rockville, |
| [23] | Masera, Taylor Barbra, & Kammen Daniel. (2000). From Linear Fuel Switching to Multiple Cooking Strategies: A Critique and Alternative to the Energy Ladder model. 28. |
| [24] | Mbatchou Ngahane BH, Nouyep J, Nganda Motto M, Mapoure Njankouo Y, Wandji A, Endale M, Afane Ze E. (2016). Post-tuberculous lung function impairment in a tuberculosis reference clinic in Cameroon. Respir Med., 114, 67-71. |
| [25] | Muazu, N. B, Ogujiubab K., Tukur H. R. (2020). Biomass Energy Dependence in South Africa: Are the Western Cape Province households descending the energy ladder after improvement in electricity access? Energy Reports, 6 (2020), 207-213. |
| [26] | Muindi, K., Murage, K. E., Egondi, T., & Rocklov, J. (2016). Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums. Toxics, 4(12), 1-13. |
| [27] | Mutua, K., Wekesa, A., & Ndungi, F. (2024). Determinants of respiratory symptoms among biomass-dependent households in rural Kenya. East African Medical Journal, 101(2), 203-215. |
| [28] | Munyao, C., Kiptoo, K., Simiyu, G., & Chelal, J. (2017). Household Air Pollutionin Rural Western Kenya: A Major Public Health Challenge. Journal of Environmental Science, Toxicology and Food Technology, 11(7), 87-96. |
| [29] | Mutahi, K., et al. (2021). Sustainable life due to indoor and outdoor air quality. Environment International, 147, 106318. |
| [30] | Nsoh, M., Olga, B., Mankollo, Y., Ebongue, M., Cyprien, K. N., Likeng, J. L. N., Islam, S. M. S., Collier, A., Mahlako, J., Gwegweni, T., & Cumber, S. N. (2019). Household indoor air quality and respiratory health of children under five. Pan African Medical Journal, 32(99), 1-8. |
| [31] | Onyeneke RU, Nwajiuba CU, Mmagu CJ, et al. (2018). Impact of adoption of improved cook-stove on different components of household welfare in rural communities in Nigeria: the case of Save80 cook-stove in Kaduna. Environ Prog Sustain Energy. 37(4): 1327-1338. |
| [32] | Person, B., Loo, D. J., Owuor, M., Ogange, L., Jefferds, M. E., & Cohen, A. (2012). “It Is Good for My Family’s Health and Cooks Food in a Way That My Heart Loves”: Qualitative Findings and Implications for Scaling Up an Improved Cookstove Project in Rural Kenya. International Journal of Environment Research and Public Health, 9(5), 1566-1580. |
| [33] | Pilishvili, T., Loo, D. J., schrag, S., Stanistreet, D., Christensen, B., Yip, F., Nyagol, R., Quick, R., Sage, M., & Nigel, B. (2016). Effectiveness of Six Improved Cookstoves in Reducing Household Air Pollution and Their Acceptability in Rural Western Kenya. PLoS ONE, 11(11), 1-17. |
| [34] | Pope DP, Mishra V, Thompson L, Siddiqui AR, Rehfuess EA, Weber M, Bruce NG (2010). Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol Rev. Pub Med, 32: 70-81. |
| [35] | Rana, J., Uddin, J., Peltier, R., & Oulhote, Y. (2019). Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter? Environmental Research and Public Health, 16(2910), 1-13. |
| [36] | Rawi, N. A. N., Jalaludin, J., & Chua, P. C. (2014). Indoor Air Quality and Respiratory Health among Malay Preschool Children in Selangor. BioMed Research International, 2015, 1-8. |
| [37] | Rehfuess, E., Pope, D., & Bruce, N. (2023). Addressing household air pollution in Africa: Women’s exposure, health risks, and policy gaps. Annual Review of Public Health, 44, 461-480. |
| [38] | Sanbata, H., Asfaw, A., & Kumie, A. (2014). Association of Biomass fuel Use With Acute Respiratory Infections Among Under- five Children in a Slum Urban of Addis Ababa, Ethiopia. BMC Public Health, 14(1122), 1-8. |
| [39] | Smith, K. R., & Pillarisetti, A. (2018). Household air pollution and health: A call for research. Journal of Environmental Science and Policy, 85, 30-38. |
| [40] | van der Kroon, B., Brouwer, R., & Van Beukering, P. J. H. (2013). The energy ladder: Theoretical myth or empirical truth? Results from a meta-analysis. 20, 504-513. |
| [41] | Wafula ST, Nalugya A, Mendoza H, Kansiime WK, Ssekamatte T, Walekhwa AW, Mugambe RK, Walter F, Ssempebwa JC, Musoke D. (2023). Indoor air pollutants and respiratory symptoms among residents of an informal urban settlement in Uganda: A cross-sectional study PLoS One. 18(8), 1-15. |
| [42] | Weldemariam, M. M., Tesfaye, A., & Kassa, H. (2023). Household fuel use and respiratory symptoms among women and adolescent girls in Ethiopia: Evidence from community health surveys. BMC Pulmonary Medicine, 23(1), 458-470. |
| [43] | Woolley, K. E., Bartington, S. E., Thomas, G. N., Pope, F. D., Muhizi, A., Mugabe, C., Ahishakiye, O., Kabera, T., & Greenfield, S. M. (2022). Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda. Sustainability, 14(3), 1-15. |
| [44] | World Health Organization. (2024). Household Air Pollution and Health: Global Update 2024. World Health Organization. |
| [45] | World Health Organization. (2022). Household Air Pollution and Health: Global Update 2022. World Health Organization. |
| [46] | World Health Organization. (2021). Household Air Pollution and Health: Global Update 2021. World Health Organization. |
| [47] | Yip, F., Christensen, B., Sircar, K., Bruce, N., Pennise, D., Lozier, M., Pilishvili, T., Farrar, J. L., Stanistreet, D., Nyagol, R., Muoki, L. de, Sage, M., & Kapil, V. (2016). Assessment of traditional and improved stove use on household air pollution and personal exposures in rural western Kenya. Environment International, 99, 185-191. |
| [48] | Zhang, D., Li, Y., Chen, Q., Jiang, Y., Chu, C., Ding, Y., Yu, Y., Fan, Y., Shi, J., Luo, Y., & Zhou, W. (2019). The relationship between air quality and respiratory pathogens among children in Suzhou City. Italian Journal of Pediatrics, 45(123), 1-10. |
APA Style
Muchend, M., Nzengya, D. M. (2026). Biomass Solid Fuel Usage and Incidences of Respiratory Symptoms Amongst Women in Households That Have Adopted ICS in Nakuru Town East Suburbs. World Journal of Public Health, 11(1), 78-91. https://doi.org/10.11648/j.wjph.20261101.20
ACS Style
Muchend, M.; Nzengya, D. M. Biomass Solid Fuel Usage and Incidences of Respiratory Symptoms Amongst Women in Households That Have Adopted ICS in Nakuru Town East Suburbs. World J. Public Health 2026, 11(1), 78-91. doi: 10.11648/j.wjph.20261101.20
@article{10.11648/j.wjph.20261101.20,
author = {Margaret Muchend and Daniel Muasya Nzengya},
title = {Biomass Solid Fuel Usage and Incidences of Respiratory Symptoms Amongst Women in Households That Have Adopted ICS in Nakuru Town East Suburbs},
journal = {World Journal of Public Health},
volume = {11},
number = {1},
pages = {78-91},
doi = {10.11648/j.wjph.20261101.20},
url = {https://doi.org/10.11648/j.wjph.20261101.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261101.20},
abstract = {One of the main causes of home air pollution, especially in developing nations, is the use of solid biomass fuels (wood, crop leftovers, animal dung, and coal) for cooking and heating. This has serious negative impacts on respiratory health. Chronic obstructive pulmonary disease (COPD), chronic bronchitis, asthma, and acute lower respiratory infections (ALRI) are all closely associated with long-term exposure to high amounts of particulate matter (PM2.5) and carbon monoxide (CO) from these fuels. The purpose of this study was to examine the Influence of biomass solid fuel usage on incidences of respiratory symptoms amongst women adopters of ICS in Nakuru town East suburbs. The study was informed by energy stacking and theory of subsidy. The study utilized mixed method research design. Data were collected from 315 female heads from of households that had adopted ICS, two FGD and key informant interviews. Sampling techniques utilized were multi-stage cluster sampling for the women heads of households while purposive sampling was used to select KIIs and participants in the FGDs. Quantitative data was analyzed using descriptive statistics and logistic regression. Qualitative data was content analyzed. Study findings revealed that 67.8% of households relied on charcoal, while 54.9% used firewood, often alongside ICS. Households that predominantly used firewood reported the highest incidence of respiratory symptoms, highlighting the persistent dangers of solid fuel combustion. Logistic regression analysis demonstrated that women in firewood-dependent households were 2.43 times more likely to experience respiratory related symptoms than those using charcoal.},
year = {2026}
}
TY - JOUR T1 - Biomass Solid Fuel Usage and Incidences of Respiratory Symptoms Amongst Women in Households That Have Adopted ICS in Nakuru Town East Suburbs AU - Margaret Muchend AU - Daniel Muasya Nzengya Y1 - 2026/03/12 PY - 2026 N1 - https://doi.org/10.11648/j.wjph.20261101.20 DO - 10.11648/j.wjph.20261101.20 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 78 EP - 91 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20261101.20 AB - One of the main causes of home air pollution, especially in developing nations, is the use of solid biomass fuels (wood, crop leftovers, animal dung, and coal) for cooking and heating. This has serious negative impacts on respiratory health. Chronic obstructive pulmonary disease (COPD), chronic bronchitis, asthma, and acute lower respiratory infections (ALRI) are all closely associated with long-term exposure to high amounts of particulate matter (PM2.5) and carbon monoxide (CO) from these fuels. The purpose of this study was to examine the Influence of biomass solid fuel usage on incidences of respiratory symptoms amongst women adopters of ICS in Nakuru town East suburbs. The study was informed by energy stacking and theory of subsidy. The study utilized mixed method research design. Data were collected from 315 female heads from of households that had adopted ICS, two FGD and key informant interviews. Sampling techniques utilized were multi-stage cluster sampling for the women heads of households while purposive sampling was used to select KIIs and participants in the FGDs. Quantitative data was analyzed using descriptive statistics and logistic regression. Qualitative data was content analyzed. Study findings revealed that 67.8% of households relied on charcoal, while 54.9% used firewood, often alongside ICS. Households that predominantly used firewood reported the highest incidence of respiratory symptoms, highlighting the persistent dangers of solid fuel combustion. Logistic regression analysis demonstrated that women in firewood-dependent households were 2.43 times more likely to experience respiratory related symptoms than those using charcoal. VL - 11 IS - 1 ER -
School of Education and Social Sciences, St Paul’s University, Limuru, Kenya
School of Education and Social Sciences, St Paul’s University, Limuru, Kenya