Traumatic brain injury (TBI) represents a significant public health challenge in sub-Saharan Africa, with limited data on outcomes in Cameroon. This prospective observational study evaluated outcomes and associated factors of TBI among adult patients treated in Buea Health District (BHD), Cameroon, from January 2020 to December 2025. A total of adult patients diagnosed with TBI were included. Data on socio-demographic characteristics, clinical severity (Glasgow Coma Scale scores), injury mechanisms, treatment pathways, and outcomes were collected using structured questionnaires and medical records. The primary outcome was functional status at discharge assessed using the Glasgow Outcome Scale (GOS), dichotomised into favourable (GOS 4–5) and unfavourable (GOS 1–3) outcomes. Statistical analysis included descriptive statistics, chi-square tests, and bivariable and multivariable logistic regression to identify independent predictors. Results showed that 74% of patients achieved favourable outcomes, with road traffic injuries (60%) being the leading cause, followed by falls (23%) and assaults (10%). Most patients were young adult males (78%), consistent with global patterns. Clinical severity indicators were strongly predictive of outcomes: patients with GCS scores 13–15 had overwhelmingly favourable outcomes (79%), while those with GCS < 8 had predominantly unfavourable outcomes (χ2 = 93.605, p < 0.001). Duration of unconsciousness >24 hours and post-traumatic amnesia were significant negative predictors (p < 0.001). Socio-demographic variables showed no significant associations with outcomes. Quality of life assessments revealed 76.5% were discharged successfully, though 23.5% experienced residual complaints, including seizures (10.5%), memory loss (4.5%), and paralysis (2%). These findings highlight that TBI in BHD predominantly affects young adult males through preventable mechanisms. Clinical severity remains the most critical outcome predictor, underscoring the need for improved pre-hospital care, timely presentation, and neurosurgical capacity to reduce the burden of TBI in Cameroon.
| Published in | World Journal of Public Health (Volume 11, Issue 3) |
| DOI | 10.11648/j.wjph.20261103.11 |
| Page(s) | 221-233 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Traumatic Brain Injury, Glasgow Outcome Scale, Affected Factors, Outcome Predictors, Cameroon
GOS Category | Outcome | Description |
|---|---|---|
1: Death | Unfavourable | Patients were certified for death. |
2: Coma | Unfavourable | The patient exhibited no obvious cortical function. |
3: Severe disability | Unfavourable | Patients were conscious but disabled; they could not perform any activity independently. |
4: Moderate disability | Favourable | Patients were disabled but independent in daily life; disabilities included varying degrees of dysphasia and hemiparesis. |
5: Good recovery | Favourable | Resumption of normal activities, even though there may be minor neurological or psychological deficits. |
Variables | Category | Favourable N (%) | Unfavourable N (%) | Total N (%) | χ2 | p-value |
|---|---|---|---|---|---|---|
Age | 18-24 | 59 (29.50) | 8 (4.00) | 67 (33.50) | 2.957 | 0.565 |
25-34 | 41 (20.50) | 3 (1.50) | 44 (22.00) | |||
35-44 | 26 (13.00) | 2 (1.00) | 28 (14.00) | |||
45-54 | 24 (12.00) | 5 (2.50) | 29 (14.50) | |||
>55 | 27 (13.50) | 5 (2.50) | 32 (16.00) | |||
Sex | Male | 141 (70.5) | 15 (7.5) | 156 (78.00) | 2.475 | 0.116 |
Female | 36 (18.00) | 8 (4.00) | 44 (22.00) | |||
Educational level | Primary | 57 (28.5) | 8 (4.00) | 65 (32.50) | 1.372 | 0.504 |
Secondary | 78 (39.00) | 12 (6.00) | 90 (45.00) | |||
Tertiary | 42 (21.00) | 3 (1.50) | 45 (22.50) | |||
Marital Status | Married | 78 (39.00) | 12 (6.00) | 90 (45.00) | 0.54 | 0.462 |
Single | 99 (49.50) | 11 (5.50) | 110 (55.00) |
Variables | Category | Favourable outcome N (%) | Unfavourable outcome N (%) | Total N (%) | χ2 | p-value |
|---|---|---|---|---|---|---|
Mechanism of injury | Assaults | 19 (9.50) | 1 (0.50) | 20 (10.00) | 7.653 | 0.054 |
Fall | 36 (18.00) | 10 (5.00) | 46 (23.00) | |||
RTI | 108 (54.00) | 12 (6.00) | 120 (60.00) | |||
Others | 14 (7.00) | 0 (0.00) | 14 (7.00) | |||
First responder | Community people | 13 (6.50) | 3 (1.50) | 16 (8.00) | 1.571 | 0.666 |
Family | 49 (24.50) | 6 (3.00) | 55 (27.50) | |||
Friends/ Colleagues | 28 (14.00) | 2 (1.00) | 30 (15.00) | |||
Pedestrians | 87 (43.50) | 12 (6.00) | 99 (49.5) | |||
Received first aid or CPR | No | 166 (83.00) | 22 (11.00) | 188 (94.00) | 0.126 | 0.723 |
Yes | 11 (5.500) | 1 (0.50) | 12 (6.00) | |||
Immobilized/ transfer | No | 164 (82.00) | 21 (10.50) | 185 (92.50) | 0.054 | 0.817 |
Yes | 13 (6.50) | 2 (1.00) | 15 (7.50) | |||
First level of contact for txt | DH | 34 (17.00) | 6 (3.00) | 40 (20.00) | 5.707 | 0.734 |
IHC | 6 (3.00) | 2 (1.00) | 8 (4.00) | |||
PH | 55 (27.50) | 10 (5.00) | 65 (32.50) | |||
RH | 82 (41.00) | 5 (2.50) | 87 (43.50) | |||
Received txt/ 1 level | No | 78 (39.00) | 12 (6.00) | 90 (45.00) | 0.54 | 0.462 |
Yes | 99 (49.50) | 11 (5.50) | 110 (55.00) | |||
Time/injury-txt | <1 hour | 76 (38.00) | 7 (3.50) | 83 (41.50) | 1.311 | 0.252 |
>8 hours | 101 (50.50) | 16 (8.00) | 117 (58.50) | |||
GCS | <8 | 5 (2.50) | 14 (7.00) | 19 (9.50) | 93.605 | 0.000 |
13-15 | 158 (79.00) | 3 (1.50) | 161 (80.50) | |||
9-12 | 14 (7.00) | 6 (3.00) | 20 (10.00) | |||
Duration consciousness (h) | <24 | 19 (9.50) | 17 (8.50) | 36 (18.00) | 55.046 | 0.000 |
>24 | 158 (79.00) | 6 (3.00) | 164 (82.00) | |||
PT-amnesia | No | 168 (84.00) | 15 (7.50) | 183 (91.50) | 23.082 | 0.000 |
Yes | 9 (4.50) | 8 (4.00) | 17 (8.50) | |||
Associated injury | Brain swollen/ contusion | 4 (2.00) | 71 (35.50) | 75 (37.50) | 6.45 | 0.168 |
BSF | 2 (1.00) | 13 (6.50) | 15 (7.50) | |||
EDH | 3 (1.50) | 30 (15.00) | 33 (16.30) | |||
Other skull fracture | 2 (1.00) | 10 (5.00) | 12 (6.00) | |||
SDH | 12 (6.00) | 53 (26.50) | 65 (32.50) |
Variables | Category | Outcome | p-value | |
|---|---|---|---|---|
AOR | 95% CI | |||
Age | 18-24 | 0.0368 | (-0.0991, 0.1728) | 0.593 |
25-34 | 0.0881 | (-0.0589, 0.2350) | 0.239 | |
35-44 | 0.0848 | (-0.0788, 0.2485) | 0.308 | |
45-54 | -0.0162 | (-0.1783, 0.1460) | 0.844 | |
>55 | Ref | Ref | ||
Sex | Female | Ref | Ref | |
Male | 0.0857 | (-0.0216, 0.1929) | 0.117 | |
Educational level | Primary | |||
Secondary | -0.0103 | (-0.1131, 0.0926) | 0.844 | |
Tertiary | 0.0564 | (-0.0661, 0.1789) | 0.365 | |
Status | Married | Ref | Ref | |
Single | 0.0333 | (-0.0564, 0.1231) | 0.465 | |
Mechanism of injury | Others | Ref | Ref | |
Assaults | -0.05 | (-0.267, 0.167) | 0.65 | |
Fall | -0.2174 | (-0.4076, -0.0271) | 0.025 | |
RTI | -0.1 | (-0.2760, 0.0760) | 0.264 | |
First responder | Community people | Ref | Ref | |
Family | 0.0784 | (-0.1014, 0.2582) | 0.391 | |
Friends/ Colleagues | 0.1208 | (-0.0751, 0.3168) | 0.225 | |
Pedestrians | 0.0663 | (-0.1043, 0.2369) | 0.444 | |
Received first aid or CPR | No | Ref | Ref | |
Yes | 0.0337 | (-0.1545, 0.2219) | 0.724 | |
Immobilized/Transfer | No | Ref | Ref | |
Yes | -0.0198 | (-0.1895, 0.1499) | 0.818 | |
First Level of Contact for TXT | DH | Ref | ||
IHC | -0.1 | (-0.343, 0.143) | 0.417 | |
PH | -0.0038 | (-0.1297, 0.1220) | 0.952 | |
RH | 0.0925 | (-0.0271, 0.2122) | 0.129 | |
Received TXT/1 Level | No | Ref | Ref | |
Yes | 0.0333 | (-0.0564, 0.1231) | 0.465 | |
Time/Injury-TXT | <1 hour | Ref | Ref | |
>8 hours | -0.0524 | (-0.1429, 0.0380) | 0.254 | |
GCS | <8 | |||
13-15 | 0.7182 | (0.6061, 0.8304) | 0.000 | |
9-12 | 0.4368 | (0.2887, 0.5850) | 0.000 | |
Duration/Consciousness/ Hrs | <24 hours | Ref | Ref | |
>24 hours | 0.4356 | (0.3366, 0.5347) | 0.000 | |
PT-Amnesia | No | Ref | Ref | |
Yes | -0.3886 | (-0.5394, -0.2378) | 0.000 | |
Associated injury | Other skull fracture | Ref | Ref | |
Brain swollen/ contusion | 0.1133 | -0.0816, 0.3082 | 0.253 | |
BSF | 0.033 | -0.209, 0.276 | 0.787 | |
EDH | 0.076 | -0.136, 0.287 | 0.48 | |
SDH | -0.0179 | -0.2149, 0.1790 | 0.858 | |
GOS | Glasgow Outcome Scale |
LMICs | Low- and Middle-income Countries |
SSA | Sub-Saharan Africa |
TBI | Traumatic Brain Injury |
HICs | High-income Countries |
RTIs | Road Traffic Incidents |
PTA | Post-traumatic Amnesia |
EDH | Epidural Hematoma |
GOSE | Glasgow Outcome Scale-Extended |
QoLIBRI | Quality of Life After Brain Injury |
BHD | Buea Health District |
STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
DAMA | Discharged Against Medical Advice |
| [1] | Feigin, V. L., Gronseth, P., & The GEO-TBI Investigators. (2022). Global epidemiology and outcomes following traumatic brain injury: Core protocol. GEO-TBI Registry. |
| [2] | Yan, J., Wang, C., & Sun, B. (2025). Global, regional, and national burdens of traumatic brain injury from 1990 to 2021. Frontiers in Public Health, 13, Article 1556147. |
| [3] | Buh, F. C., Sumbele, I. U. N., Maas, A. I. R., Motah, M., Pattisapu, J. V., Youm, E., Meh, B. K., Kobeissy, F. H., Wang, K. W., Hutchinson, P. J. A., & Taiwe, G. S. (2023). Traumatic brain injury in Cameroon: A prospective observational study in a Level I trauma centre. Medicina, 59(9), 1558. |
| [4] | Adegboyega, G., Zolo, Y., Sebopelo, L. A., Dalle, D. U., Dada, O. E., Mbangtang, C. B., Tetinou, F., Kanmounye, U. S., & Alalade, A. F. (2021). The burden of traumatic brain injury in Sub-Saharan Africa: A scoping review. World Neurosurgery, 156, e192–e205. |
| [5] | Eaton, J., Hanif, A. B., Grudziak, J., & Charles, A. (2017). Epidemiology, management, and functional outcomes of traumatic brain injury in Sub-Saharan Africa. World Neurosurgery, 108, 650–655. |
| [6] | Molla, Y. D., & Alemu, H. T. (2025). Epidemiology of traumatic brain injury in Ethiopia: A systematic review and meta-analysis of prevalence, mechanisms, and outcomes. PLoS One, 20(5), e0322641. |
| [7] | Maas, A. I. R., Menon, D. K., Adelson, P. D., & Narayan, R. K. (2017). Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. The Lancet Neurology, 16(12), 987–1048. |
| [8] | Wells, A. J., & Reilly, P. L. (2025). 50 years of the Glasgow Coma Scale: A historical perspective. Journal of Clinical Neuroscience, 133, Article 110994. |
| [9] | G/Michael, S., Terefe, B., Asfaw, M. G., & Liyew, B. (2023). Outcomes and associated factors of traumatic brain injury among adult patients treated in Amhara regional state comprehensive specialized hospitals. BMC Emergency Medicine, 22(2), 1. |
| [10] | Malhotra, A. K., Shakil, H., Smith, C. W., Huang, Y. Q., Kwong, J. C., Thorpe, K. E.,. & Nathens, A. B. (2025). Predicting outcomes after moderate and severe traumatic brain injury using artificial intelligence: A systematic review. npj Digital Medicine, 8(1), 373. |
| [11] | Pavlovic, D., Pekic, S., Stojanovic, M., & Popovic, V. (2019). Traumatic brain injury: Neuropathological, neurocognitive and neurobehavioral sequelae. Pituitary, 22(3), 270–282. |
| [12] | Davis, K. C., Slomine, B. S., Salorio, C. F., & Suskauer, S. J. (2016). Time to follow commands and duration of posttraumatic amnesia predict GOS-E Peds scores 1 to 2 years after TBI in children requiring inpatient rehabilitation. Journal of Head Trauma Rehabilitation, 31(2), E39–E47. |
| [13] | Koipapi, S., Mmbaga, B. T., Chilonga, K., Msuya, D., Rabiel, H., Nkoronko, M.,. & Chugulu, S. (2024). Outcomes of traumatic brain injury patients with acute epidural and subdural hematoma who underwent burr hole surgery: A two-year study at Kilimanjaro Christian Medical Centre, Tanzania. World Neurosurgery: X, 21, Article 100257. |
| [14] | Taalas, W., Raj, R., Öhman, J., & Siironen, J. (2023). Long-term functional outcome and quality of life in long-term traumatic brain injury survivors. Neurotrauma Reports, 4(1), neur-2023. |
| [15] | Ansari, A., Zoghi, S., Feili, M., Azad, T. D., Mousavi, S. R., Niakan, A.,. & Khalili, H. (2025). The impact of Glasgow Outcome Scale-Extended cut-point of dichotomization on factors associated with outcomes in traumatic brain injury research. Neurosurgical Review, 48(1), 767. |
| [16] | Zimmerman, A., Fox, S., Griffin, R., Nelp, T., Thomaz, E. B. A. F., Mvungi, M.,. & Sica, R. (2020). An analysis of emergency care delays experienced by traumatic brain injury patients presenting to a regional referral hospital in a low-income country. PLoS ONE, 15(10), e0240528. |
| [17] | Muili, A. O., Kuol, P. P., Jobran, A. W., Lawal, R. A., Agamy, A. A., & Bankole, N. D. A. (2024). Management of traumatic brain injury in Africa: Challenges and opportunities. International Journal of Surgery, 110(6), 3760–3767. |
| [18] | Buh, F. C., Taiwe, G. S., Maas, A. I. R., Motah, M., Youm, E., Wanyu, B. Y., Wang, K. W., Hutchinson, P. J. A., & Sumbele, I. U. N. (2022). Demographics, causes, and outcome of traumatic brain injury among trauma cases in Cameroon: A multi-center five year’s retrospective study. Neurotrauma Reports, 3(1), 570-583. |
| [19] | Arora, S., Ong, A., Wilkes, M., Aralis, H., & Sciolla, A. F. (2025). Trauma and resilience in an urban clinic for unhoused young adults: A mixed methods study. PLOS Mental Health, 2(9), e0000392. |
| [20] | Singh, A., & Mukherjee, S. (2024). Exploring the influence of childhood trauma on resilience and mental health outcomes among emerging adults. International Journal of Humanities Social Science and Management (IJHSSM), 4(3), 654–662. |
| [21] | Ngu, C. N., Shete, P., Nsagha, D. S., Tanue, E. A., Tendongfor, N., Oke, R., Bassah, N., Ukah, C. E., McCoy, S. I., Juillard, C., Mefire, A. C., & Ekane, E. G. H. (2025). Epidemiological profile of road traffic injury patients, and post-traumatic stress disorder (PTSD) screening uptake in hospitals in Fako Division, Cameroon. PLOS Global Public Health, 5(12), e0004847. |
| [22] | Ngekeng, S., Kibu, O., Oke, R., Bassah, N., Touko, D. A., Yost, M. T., Dissak-Delon, F., Tendongfor, N., Nguefack-Tsague, G., Hubbard, A., McCoy, S. I., Christie, S. A., Chichom-Mefire, A., & Juillard, C. (2024). Prehospital factors associated with mortality among road traffic injury patients: Analysis of Cameroon trauma registry data. BMC Emergency Medicine, 24(1), 194. |
| [23] | Kobusingye, O. C., Hyder, A. A., Bishai, D., Hicks, E. R., Mock, C., & Joshipura, M. (2005). Emergency medical systems in low- and middle-income countries: Recommendations for action. Bulletin of the World Health Organization, 83(8), 626–631. |
| [24] | Mock, C., Arreola-Risa, C., & Quansah, R. (2003). Strengthening care for injured persons in less developed countries: A case study of Ghana and Mexico. Injury Control and Safety Promotion, 10(1–2), 45–51. |
| [25] | Chou, R., Totten, A. M., Pappas, M., Carney, N., Dandy, S., Grusing, S., Fu, R., Wasson, N., & Newgard, C. (2017). Glasgow Coma Scale for field triage of trauma: A systematic review (Comparative Effectiveness Review No. 182). Agency for Healthcare Research and Quality. |
| [26] | Maas, A. I. R., Stocchetti, N., & Bullock, R. (2008). Moderate and severe traumatic brain injury in adults. The Lancet Neurology, 7(8), 728–741. |
| [27] | Banoei, M. M., Hutchison, J., Panenka, W., Wong, A., Wishart, D. S. & Winston, B. W (2025). Metabolomic in severe traumatic brain injury: exploring primary, secondary injuries, diagnosis, and severity. Critical Care, 29: 26. |
| [28] | Nkouonlack, C., Arnuld, M., Chunteng, N., Mefire, C. (2023). Determinants of outcomes in patients with traumatic brain injury in Buea and Limbe regional hospitals, south west region, Cameroon: A 5-year retrospective study. Journal of the neurological Sciences, 455. |
| [29] | Majdan, M., Plancikova, D., Brazinova, A., Rusnak, M., Nieboer, D., Feigin, V., & Maas, A. (2016). Epidemiology of traumatic brain injuries in Europe: A cross-sectional analysis. The Lancet Public Health, 1(2), e76–e83. |
| [30] | Rafiee, S., Baratloo, A., Safaie, A., Jalali, A., & Komlakh, K. (2022). The outcome predictors of the patients with traumatic brain injury: A cross-sectional study. Bulletin of Emergency Trauma, 10(4), 165–171. |
| [31] | Eghzawi, A., Alsabbah, A., Gharaibeh, S., Alwan, I., Gharaibeh, A., & Goyal, A. V. (2024). Mortality predictors for adult patients with mild-to-moderate traumatic brain injury: A literature review. Neurology International, 16(2), 406–418. |
| [32] | Schüller, D., Wafaisade, A., Lefering, R., Migliorini, F., Bolierakis, E., Weuster, M., Kubo, Y., Fröhlich, M., & Driessen, A., on behalf of the Trauma Register DGU. (2026). Predictive Accuracy of Glasgow Coma Scale and Pupillary Data on Presence of Traumatic Brain Injury. Journal of Clinical Medicine, 15(2), 697. |
| [33] | Vella, M. A., Patel, M., & Patel, M. B. (2017). Acute management of traumatic brain injury. Surgical Clinics of North America, 97(6), 1015–1030. |
| [34] | Haas, B., Stukel, T. A., Gomez, D., Zagorski, B., De Mestral, C., Sharma, S. V., Rubenfeld, G. D., & Nathens, A. B. (2012). The mortality benefit of direct trauma center transport in a regional trauma system: A population-based analysis. Journal of Trauma and Acute Care Surgery, 72(6), 1510–1515. |
| [35] | Goldschlager, T., Rosenfeld, J. V., & Winter, C. D. (2007). ‘Talk and die’ patients presenting to a major trauma centre over a 10 year period: A critical review. Journal of Clinical Neuroscience, 14(7), 618–623. |
| [36] | Thompson, H. J., McCormick, W. C., & Kagan, S. H. (2006). Traumatic brain injury in older adults: Epidemiology, outcomes, and future implications. Journal of the American Geriatrics Society, 54(10), 1590–1595. |
| [37] | Rickels, E. (2017). Focus on traumatic brain injury. European Journal of Trauma and Emergency Surgery, 43(6), 729–730. |
| [38] | Hoffmann, M., Lefering, R., Rueger, J. M., Kolb, J. P., Izbicki, J. R., Ruecker, A. H., Rupprecht, M., & Lehmann, W. (2012). Pupil evaluation in addition to Glasgow Coma Scale components in prediction of traumatic brain injury and mortality. British Journal of Surgery, 99(1), 122–130. |
| [39] | Brennan, P. M., Murray, G. D., & Teasdale, G. M. (2018). Simplifying the use of prognostic information in traumatic brain injury. Part 1: The GCS-Pupils score: An extended index of clinical severity. Journal of Neurosurgery, 128(6), 1612–1620. |
APA Style
Akwo, N. S., Bate, D. O., Fomanka, E. E., Enow, E. N. B., Smith, N. E., et al. (2026). Outcomes and Associated Factors of Traumatic Brain Injury Among Adult Patients Treated in Buea Health District (BHD), Cameroon. World Journal of Public Health, 11(3), 221-233. https://doi.org/10.11648/j.wjph.20261103.11
ACS Style
Akwo, N. S.; Bate, D. O.; Fomanka, E. E.; Enow, E. N. B.; Smith, N. E., et al. Outcomes and Associated Factors of Traumatic Brain Injury Among Adult Patients Treated in Buea Health District (BHD), Cameroon. World J. Public Health 2026, 11(3), 221-233. doi: 10.11648/j.wjph.20261103.11
@article{10.11648/j.wjph.20261103.11,
author = {Nnoko Sona Akwo and David Oben Bate and Esembieng Esua Fomanka and Enow Nkah Bruno Enow and Ntungwe Ekwelle Smith and Oben Joan Ayuk and Yoah Aldof Tah and Kingsley Enow Nkongho and Maxwell Kofi Danso and Isaac Obeng Gyasi and Emeh Nathan Agbor},
title = {Outcomes and Associated Factors of Traumatic Brain Injury Among Adult Patients Treated in Buea Health District (BHD), Cameroon},
journal = {World Journal of Public Health},
volume = {11},
number = {3},
pages = {221-233},
doi = {10.11648/j.wjph.20261103.11},
url = {https://doi.org/10.11648/j.wjph.20261103.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261103.11},
abstract = {Traumatic brain injury (TBI) represents a significant public health challenge in sub-Saharan Africa, with limited data on outcomes in Cameroon. This prospective observational study evaluated outcomes and associated factors of TBI among adult patients treated in Buea Health District (BHD), Cameroon, from January 2020 to December 2025. A total of adult patients diagnosed with TBI were included. Data on socio-demographic characteristics, clinical severity (Glasgow Coma Scale scores), injury mechanisms, treatment pathways, and outcomes were collected using structured questionnaires and medical records. The primary outcome was functional status at discharge assessed using the Glasgow Outcome Scale (GOS), dichotomised into favourable (GOS 4–5) and unfavourable (GOS 1–3) outcomes. Statistical analysis included descriptive statistics, chi-square tests, and bivariable and multivariable logistic regression to identify independent predictors. Results showed that 74% of patients achieved favourable outcomes, with road traffic injuries (60%) being the leading cause, followed by falls (23%) and assaults (10%). Most patients were young adult males (78%), consistent with global patterns. Clinical severity indicators were strongly predictive of outcomes: patients with GCS scores 13–15 had overwhelmingly favourable outcomes (79%), while those with GCS 2 = 93.605, p 24 hours and post-traumatic amnesia were significant negative predictors (p < 0.001). Socio-demographic variables showed no significant associations with outcomes. Quality of life assessments revealed 76.5% were discharged successfully, though 23.5% experienced residual complaints, including seizures (10.5%), memory loss (4.5%), and paralysis (2%). These findings highlight that TBI in BHD predominantly affects young adult males through preventable mechanisms. Clinical severity remains the most critical outcome predictor, underscoring the need for improved pre-hospital care, timely presentation, and neurosurgical capacity to reduce the burden of TBI in Cameroon.},
year = {2026}
}
TY - JOUR T1 - Outcomes and Associated Factors of Traumatic Brain Injury Among Adult Patients Treated in Buea Health District (BHD), Cameroon AU - Nnoko Sona Akwo AU - David Oben Bate AU - Esembieng Esua Fomanka AU - Enow Nkah Bruno Enow AU - Ntungwe Ekwelle Smith AU - Oben Joan Ayuk AU - Yoah Aldof Tah AU - Kingsley Enow Nkongho AU - Maxwell Kofi Danso AU - Isaac Obeng Gyasi AU - Emeh Nathan Agbor Y1 - 2026/07/08 PY - 2026 N1 - https://doi.org/10.11648/j.wjph.20261103.11 DO - 10.11648/j.wjph.20261103.11 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 221 EP - 233 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20261103.11 AB - Traumatic brain injury (TBI) represents a significant public health challenge in sub-Saharan Africa, with limited data on outcomes in Cameroon. This prospective observational study evaluated outcomes and associated factors of TBI among adult patients treated in Buea Health District (BHD), Cameroon, from January 2020 to December 2025. A total of adult patients diagnosed with TBI were included. Data on socio-demographic characteristics, clinical severity (Glasgow Coma Scale scores), injury mechanisms, treatment pathways, and outcomes were collected using structured questionnaires and medical records. The primary outcome was functional status at discharge assessed using the Glasgow Outcome Scale (GOS), dichotomised into favourable (GOS 4–5) and unfavourable (GOS 1–3) outcomes. Statistical analysis included descriptive statistics, chi-square tests, and bivariable and multivariable logistic regression to identify independent predictors. Results showed that 74% of patients achieved favourable outcomes, with road traffic injuries (60%) being the leading cause, followed by falls (23%) and assaults (10%). Most patients were young adult males (78%), consistent with global patterns. Clinical severity indicators were strongly predictive of outcomes: patients with GCS scores 13–15 had overwhelmingly favourable outcomes (79%), while those with GCS 2 = 93.605, p 24 hours and post-traumatic amnesia were significant negative predictors (p < 0.001). Socio-demographic variables showed no significant associations with outcomes. Quality of life assessments revealed 76.5% were discharged successfully, though 23.5% experienced residual complaints, including seizures (10.5%), memory loss (4.5%), and paralysis (2%). These findings highlight that TBI in BHD predominantly affects young adult males through preventable mechanisms. Clinical severity remains the most critical outcome predictor, underscoring the need for improved pre-hospital care, timely presentation, and neurosurgical capacity to reduce the burden of TBI in Cameroon. VL - 11 IS - 3 ER -
Department of Occupational Health and Safety (OEH), University of Buea, Buea, Cameroon
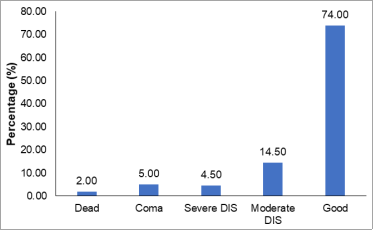
Figure 1. Outcome of Traumatic brain injury among patients treated in Buea district hospitals 2020-2025.
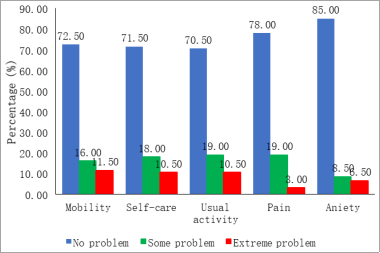
Figure 2. Quality of live after management of Traumatic brain injury among adult patients treated in Buea district hospitals 2020-2025.
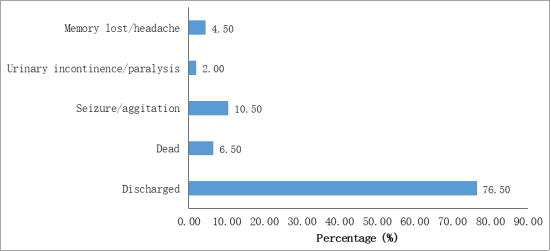
Figure 3. Other residual complains after management of Traumatic brain injury among adult patients treated in Buea district hospitals 2020-2025.
Information

